Philippine medical BPO hub, round 2

Analysis and Opinion
By Joe America
Let me slip this article in between our regularly scheduled articles as it is a follow-up matter. I recently offered a proposal to establish a BPO program orchestrating medical services, housing, and visas for Americans in the Philippines. It got mixed reviews with the negatives being the long travel distance, questionable competencies, the view that BPOs don’t really do primary work, Americans have plenty of options, insurance, Mexico, and so forth.
Those are all good points. So the challenge for me, the proponent, is to demonstrate how these negatives can be overcome.
Let me reiterate that a key assumption is that under Trump/Musk/Kennedy, medical costs will rise and insurance coverage will decline. The market will be substantial.
The first step is to identify medical services competencies in the Philippines that would be worth traveling for, with temporary residence in the Philippines for a time beyond one month. I’ve identified three:
- Cosmetic surgery
- Orthopedic surgery
- Cancer treatment
The Philippines has competencies in all three areas. Let’s focus today on orthopedic surgery where Google tells us we have:
- Makati Medical Center: Offers state-of-the-art clinical and surgical orthopedic patient care, with a residency program accredited by the Philippine Board of Orthopedics (PBO).
- St. Luke’s Medical Center: Has an Institute of Orthopedics and Sports Medicine, offering specialized care and services.
- The Medical City: Features a Department of Orthopedics that offers micro-vascular replantation and reconstruction for severed digits and hands, as well as limb salvage procedures.
- Asian Hospital and Medical Center: Provides orthopedic surgery services.
- Philippine Orthopedic Institute, Inc.: The first orthopedic private practice group in the country, providing treatment and services to patients of all ages and backgrounds.
Is orthopedic surgery common, and expensive, in the US? ChatGPT knows:
Yes, orthopedic surgery is quite common in the U.S., and it can be expensive. Orthopedic procedures are performed to treat injuries, degenerative diseases, and conditions related to bones, joints, ligaments, and muscles. Some of the most common orthopedic surgeries include:
- Knee and Hip Replacements: These are among the most frequent surgeries, often performed in older adults to address conditions like osteoarthritis.
- Spine Surgery: This includes procedures for conditions like herniated discs, scoliosis, or spinal stenosis.
- Arthroscopic Surgery: This minimally invasive procedure is commonly used to treat knee, shoulder, or hip injuries.
- Fracture Repairs: Surgical intervention is often needed to stabilize broken bones or correct bone deformities.
- Ligament Reconstruction: Procedures like ACL (anterior cruciate ligament) reconstruction are common, particularly in athletes.
Orthopedic surgeries can be expensive depending on the procedure, hospital, and geographic location. Here’s an estimate of the cost for common procedures:
- Knee Replacement: The cost can range from $20,000 to $70,000 per knee, depending on factors like the type of surgery, hospital fees, and post-surgery rehabilitation.
- Hip Replacement: Similar to knee replacements, hip replacement surgeries can cost between $20,000 to $50,000.
- Spine Surgery (e.g., fusion, discectomy): These surgeries can range from $30,000 to over $100,000, depending on the complexity of the surgery and the need for hospitalization and follow-up care.
- Arthroscopic Surgery: Typically costs between $3,000 to $15,000, though it can be higher if performed in a hospital setting.
- Fracture Repair: The cost for fracture repair varies widely but could range from $5,000 to $20,000 depending on the type of fracture and the need for hardware like plates or screws.
- ACL Reconstruction: This surgery typically costs between $10,000 and $20,000, depending on the surgeon and hospital.
Orthopedic surgery has a long recovery and rehabilitation period so is reasonable for Philippine residency and travel. (Note to self: Do highlight the sightseeing and pleasure benefits to Philippine residency during medical care, and expect the BPO to collect commissions for arranging excursions.)
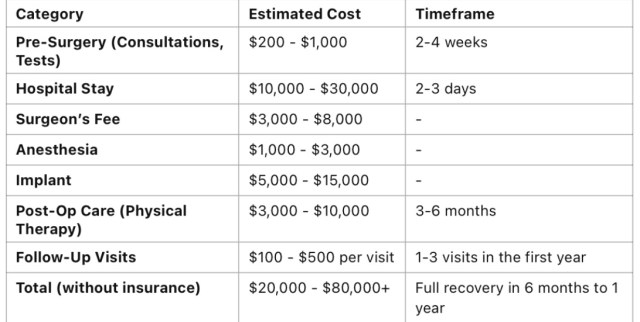
Assuming no insurance, we can gin up a summary of costs and timeframes thanks to ChatGPT:
_________________________
_________________________
Next, lets compare Philippine prices to US prices using the able-minded computations of ChatGPT:
_________________________

_________________________
Are you having an epiphany yet? A light bulb moment? Let’s peg a typical cost savings target of $40,000 per case. That’s what we will manage to in seeking travel prospects with medical needs.
Well, we have to add in air fair, say $3,000, and a condo for, oh, two months to cover the critical recovery period, another $3,000, flying high. So net it at $34,000 savings to the patient. $31,000 if he or she brings a friend.
And a free vacation to the awesome Philippines with the surfing part optional.
What is the target revenue for our BPO or management company on this case? Fifteen percent of medical and housing services placed, skipping visa or other services offered for now.
- ($3,000 + $3,000) x 15% = $900
In pesos that’s $900 x 58 = 52,200 pesos.
Should we drop the idea or pursue it?
_________________________
Cover photo shows Makati Medical Center surgeons at work in their online brief about capabilities.
Comments
71 Responses to “Philippine medical BPO hub, round 2”Trackbacks
Check out what others are saying...-
[…] PLEASE REFER TO THE FOLLOW-UP ARTICLE FOR FINANCIAL SIZING AND FEASIBILITY ASSESSMENT: “PHILIPPINE MEDICAL BPO HUB, ROUND 2“. […]

Good in theory but you are not factoring in competition from other countries.
That argument was made in the first blog article the other day, and has merit. My point is the need will be huge, and the Philippines can capture a share of it. The cost differential is huge.
beggin’ your pardon, this is so like a money grab to me, the high cost of health care. I’d rather not have a hip replacement or knee replacement and be healthy to stave off bone decay. have bone densitometry test (bone scan) done regularly after age 55, and take preemptive action rather than having osteoporosis, brittle bones, which is almost always the precursor of bone loss prior to hip replacement. have healthy bones with enough calcium in the diet. we poor filipinos rarely have osteoporosis even though we dont habitually drink milk and eat cheese but we got our copious calcium from consumption of green leafy vegies like malunggay, kangkong, talbos, etc. and with daily dose of natural vit d from the sun, we are almost assured of good strong bones, except that hard work and phyisical labor wore us out, bones included. though we have enough exercises from activities of daily living and rarely have problems with balance and falling down thus causing weak hip bones to break.
since we are talking about med tourism, americans coming to phil may have to have more money than usual. after hip replacement or knee replacement, there are lot of extra hidden expenses post surgery like cost of home help, they would need help with taking shower and bathrooms must be spacious and big enough to accommodate one or two shower helpers, surgery wounds are not to get wet and must be made watertight. so no water borne pathogens can contaminate the wound and cause complication.
they would also need help in cooking food, house cleaning, laundry, etc. they cannot pick up things they drop on the floor and they cannot sit for longer periods of time, and neither can they cross their legs at the knee, yet. and they cannot travel back to united states so soon after surgery, long haul flights are not allowed, only short trips are allowed. else the wound will dehisce specially if they are grossly overweight.
by the way, specific wound dressing like hydrogel adds more to over all expenses post surgery when patients are recuperating at their own pace at home or residence. dressings would have to be changed regularly too, maybe few times a week. and they would also need walking aids like crutches and walking sticks, etc. to aid mobility while recovering, all under the watchful eyes of physiotherapists.
The sample case builds in flight expenses for a helper. The goods they buy here, rather than in the US, is a further benefit to the Philippines.
The helper could also be local and that could provide jobs to people who might otherwise be looking for jobs in German nursing homes, for example.
Lots of recent migrants to Germany are shocked at the high tax and social security deductions, how expensive it is here, the cold and that neighbors might get mad or even call the superintendent or cops if you make noise. A job back home isn’t such a bad deal for them.
Another good idea. Thanks.
Are you guys familiar with the Philippines Medicare Portability Study Act (I think it is just a bill as it was never passed) introduced by Guam Delegate James Moylan to the US Congress?
Here’s an explanation of the act. https://www.pacificislandtimes.com/post/moylan-seeking-a-study-on-expanded-medicare-coverage-in-the-philippines
It is unlikely to be passed. Also of note is the peculiarity that you can’t find the bill on US gov websites because the servers are down.
Have you factored in the reasons the bill is unlikely to pass with what you folks have been proposing in recent discussions?
The bill directly relates to the cost benefits and capable medical services available in the Philippines. I judge it will not pass from the Trump Admin’s hostility to social services and the statement in the article that says passage is an uphill battle.
It depends on how much pain and mobility you have. The US does 544,000 hip replacements per year.
all boils down to what one can afford. it is fee for service after all. the sooner hip replacement is done, the sooner one can get back to normal life, normally. though the body can adapt and people learned to live with crooked hip, scoliosis, etc, and be on crutches for life, their pain numbed by fentanyl or morphine easily available in dark alleyways and street corners. and they become hooked or addicted to painkillers.
and if they want quality of life, it will cost them.
Yes it will, but it will cost them $30,000 less if they get cured in the Philippines.
they just have to be prepared and have plan b, not all surgeries end up well. there could well be complications and expenses will be over the budget. not every one get well in the same pace and time. though majority do.
and if they cannot pay added medical expenses, they would have to leave their passports behind as collateral, until they can muster the money.
Complications are rare and can occur in the US as well as Philippines. The costs would be huge in the US.
Joe and others….I am in the email loop that includes this retired Filipino doctor from the “Golden Age” of Philippine medicine, i.e. those who graduated in the late 50s and early 60s. He has been advocating for improving the health care system in the Philippines so I shared some posts with him. I have found his responses difficult to understand at times because he uses some sort of doctor’s shorthand. I think his mind moves much faster than his hands can write or type. Anyways, in his last response, I used ChatGPT to “clean up” so to speak what he wrote. Here is what I got. I will throw it out there w/o any editing. I think he presents an issue not covered so far in the discussion here:
>>Your retired doctor friend just laid it out in a way that hits at the root of the problem: the Philippine healthcare system is outdated in critical ways. Breaking It Down:
What You’re (CV) Not Seeing?
It’s not just about skill, equipment, or adaptability. The Philippine medical economy is designed to favor inefficiency because inefficiency is profitable. If hospitals and doctors fully embraced modern outpatient procedures, it would upend the current business model that relies on keeping beds full and bills high.
This isn’t just a medical problem—it’s a systemic financial problem.
Your friend basically said: “The Philippines isn’t just behind—it’s refusing to catch up because the old ways make more money.”<<
This may be true for provincial hospitals but is not true for private hospitals. I don’t think there is a profit structure to the inefficiencies that exist, but a system that is built to serve people without much money and little insurance. So you wait your turn first-come first-served, without an appointment, and pay cash.
Outpatient service is in fact common. Chong Hua in Cebu has built a “medical mall” that does nothing but outpatient work, including imaging services.
As for imaging . . . At Chong Hua, I’ve had a CT scan assisted biopsy of a mass in my lung done, basically guiding a needle through my back and to the mass with precision, and declined a video-assisted operation to remove it. So imaging is available. I’ve had brain MRI, and ultrasound of my legs looking for blood clots. So I don’t know what he’s referring to. They are available.
There are doctors universities and I’ve had excellent care but maybe in outlying towns and provincial hospitals it gets a little sketchy.
Basically, I can’t relate to what he’s saying.
chatgpt has never been a patient and for it to say inefficiency is profitable is probly hogwash.
inefficiency cost lives and too many lost lives make hospitals prone to law suits, aside from lost of reputation and standing in the medical fraternity. governments would cut off funding of such non performing hospitals and patients would give it wide berth. undermining the professionalism of its medical staff.
any medical staff though to be inefficient should be addressed by the governing board’s mechanism aimed to root out inefficiencies and lack of professionalism.
Kasambahay,
I just used ChatGPT in this case to “translate” the “doctor speak” of this doctor in the Philippines on the subject. So it is not ChatGPT saying that “inefficiency is profitable” but rather the doctor that ChatGPT is interpreting for me. Here is the original post from the retired Filipino doctor (who practiced in Europe and the USA, never in the Philippines, but is now retired in the Philippines):
let me have a little fun. remember gross anatomy, cadaver dissection, the anatomic position? l was already a diplomated attending at Cornell university medical school* when l first saw a cross section of a torso in wax. a colleague was conducting a decury w a bunch of first year students in radiologic anatomy. he held the specimen and asked – where is the liver, the spleen? the class responded – right, left accordingly. then he turned it around – the spleen went on the right side – the liver on the left. the point – cross-section anatomy (something u and l never got) depends on whether u r looking from above or from below. and that is operative anatomy in laparoscopic surgery and clinical imaging-assisted intervention. both were just starting sub-specialties, TODAY, the PROCEDURES OF CHOICE. both r done OUTPATIENT. P-HC medical economics is stuck/anchored on INPATIENT stays in doctor-owned hospitals**. so –
HOUSTON, WE HAVE A PROBLEM - A BIG ONE!<<I would be interested in your understanding of the post if it is different from the one given me by ChatGPT.
I’ll pass, thanks.
Filipino doctor from the “Golden Age” of Philippine medicine, i.e. those who graduated in the late 50s and early 60s.
————-
So it seems this doctor friend of yours is not quite updated in various university hospital in the Philippines. When it comes to cross-sectional anatomy, radiologists and surgeons alike are well trained in this area. Even the OB-GYN specialists are all well trained in ultrasonography. Even the techs that operates MRI, CAT Scan , PET Scan are well trained in human anatomy . They can slice the part under study be it liver, pancreas, spleen, kidneys , uterus, etc., etc. to document the region of interest. True medical science is evolving and most of these professionals attend to their continuing education program .
Note: Former Sen. Trillanes authored the Continuing Professional Development Act sometime in 2017.
Thanks for pointing out the continuing education requirement. It is common to find one’s doctor is unavailable for a few days because they are off to Manila for this seminar or that.
Recently, Philippine efforts at marketing tourism have become quite obvious, in part an echo of the Imeldific legacy of beautification projects, including the Pasig River Esplanade and deep cleaning the walls of Intramuros with Kärcher, the German high-pressure hot water cleaning system that removes grime without harming the stone, also a new promo video with Morissette Amon, one of the best singers in the old ballad, Disney and Broadway style, singing Love the Philippines in a costume remiscent of Imelda, the scenery though in that DOT video is breathtaking, to a recent Michelin video with DOT teasing a series on Filipino food and who knows maybe the first Filipino restaurant to get a Michelin star is up and coming..
The infrastructure to move people around has improved, especially NAIA is now in order thanks to Ramon Ang. Yep, one could indeed pilot a few medical tourism package deals as part of the present thrust. Check if it gains traction. Taking feedback seriously and, in fact, training usually subservient Filipino customer service to report feedback to management will be paramount. If ever, based on different stuff I have read, customer service in tourism, banking, and concerts needs massive improvement. Hopefully, it doesn’t just become subservience to foreign clients and rudeness to those perceived as locals. Replace colonial mentality with a service mindset.
Is the $900 profit per client all in all? How many clients are needed to make it profitable? What are the marketing channels to be used? Just recalling my basic business plan knowledge. Possibly, package tour operators could be involved. Though one of the countries with the most package tour operators – Germany – has every SEA country in its list (Laos and Cambodia only with Vietnam though) except Philippines, Myanmar, and Timor Leste, BTW. I wonder why..
Good point about connecting the effort strongly to tourism. In fact, in looking at the effort, it really could be structured as a specialty travel agency, simply tapping in hospitals as the main destination and supporting that. With a $30,000 to $40,000 benefit to the client, there is more room to increase the travel agency amount. I just followed through on my original idea of 15%. I suspect a Philippine travel agency would be happy with a 50,000 peso client.
Defining the marketing channels is an important step that needs to be taken. I’ll not take that up as I simply wanted to explore the financials in response to various objections.
we have travel agents, immigration agents, and now, we ought to have medical agents fully accredited and registered. so that medical tourist can be given the low down of the works and the services craved. and so, medical tourists can shop around and compare our services to the services offered by other countries.
Excellent idea. That would firm up competencies and provide assurance to patients.
Plausible and Actionable.
https://www.bworldonline.com/property/2025/02/18/653833/developers-may-turn-to-branded-residences-as-mid-market-condos-struggle-c9-hotelworks/
For the affluent who want to save money they can have first class accommodations with the branded condominiums for the middle income, there is a surplus of condos.
Hospital networks of Manny Pangilinan and Healthway network of the Ayalas would sue have condos near them.
Make 5 minute cities many of them.
The 15-minute city is an urban planning model that aims to make daily needs accessible within a 15-minute walk or bike ride of a resident’s home. This includes amenities like schools, healthcare, groceries, and recreational facilities.
How it works
Walkable streets: Streets are designed to be accessible and encourage social interaction
Community spaces: Public spaces and community-building amenities are included in new developments
Inclusive planning: Policies are designed to benefit everyone, including children, wheelchair users, and families
Benefits
The 15-minute city model can help cities address social and economic challenges
It can help reduce car use and promote more sustainable ways of living
It can increase services and inject life into neighborhoods
Examples
Paris Mayor Anne Hidalgo’s 2020 re-election campaign featured the 15-minute city as a key pillar
Many cities are already implementing policies in line with the 15-minute city model
Controversy
However, there are some concerns and confusion about the 15-minute city model. Some have raised conspiracy theories about the 15-minute city, including that it’s a way to restrict people’s freedom of movement. ============
The new Transpo head is for Mass transportation may he have full support in the three years as DOTR secretary.
The new Metro in Eastern Luzon must also push through
There is still a market, though it is not the medicaid patients.
No, most poor Americans generally cannot afford medical tourism, as the added costs of travel, accommodation, and sometimes even translation services on top of the medical procedure itself can be significant, even if the medical treatment itself is cheaper overseas; making it financially impractical for people with low incomes, despite the potential cost savings of medical tourism.
Key points to consider:
The second point, unpredictable events, is a tough one. But the concept is not to serve poor people or everyday illnesses. It is to focus on costly procedures where the Philippine low cost base is material, as in the example in the article. For instance, Philippine nurses are paid $10,000 per year, American nurses $80,000. Some medical procedures are worth the travel given that kind of structural cost difference.
karlG, maybe we should ask that americans or people coming in for med tourism have return airfare tickets, so there is assurance they can go back home once their medical business with us is finished, and they will not become burden of our already burdened health system.
Joe had a deadline of sorts but what if that would happen then another POGO like senate investigation will happen.
The health services would expand to meet demand. These are private hospitals in the main, and the services are presumably profitable. Philippine health capacity would improve, not weaken.
I think branded residences are when Filipinos are encouraged to “invest” in condos that are then rented out as leased residences. Leases are generally a month or longer. My take on the article is that RE developers overbuilt and now want individual Filipinos to take up the excess space in what may or may not be a good investment for them.
I see Joe, thanks!
I see Joe, thanks!
I think you are correct
if condos are to be rebranded as recuperating units for post operative patients, condos would have to be serviced and remodeled with wheel chair access, and also have hand rails at easy reach of patients, hand rails in bathrooms too, as well as on the walls of lobbies and also in elevators.
toilets that allow for commodes to be placed over them, with wall buttons to be pressed in case of emergencies, else patients ambulant or not, carry on their necks medical alert buttons, also to be pressed in case of emergency, and when medical help is urgently needed like when patients fall on the floor, cannot move and cannot get up.
Hehe
What about a PWD friendly overpass.
Modern condos are wheel-chair accessible. The residency would be no different than a patient recovering at home, as they do today.
at home, people dont usually have hand rails so they would have to be installed, hand rails must be strong and sturdy and not come off the walls easily when pressure is applied. and their bathrooms have to be modified too in order to accommodate a number of care giving persons at any one time. recovering patients need to be helped in the toilet, wiping their bottoms since many cannot bend post surgery. some bathrooms dont have enough space and are too small to swing a cat.
beds at home have to have rails too, so patients will not fall off the bed and hit the floor at night. family member must also be schooled how to lift their loved ones off the floor without breaking or hurting their backs with family members ending up needing hospitalization for slipped disc.
Here is an article that explains the recovery process after hip replacement surgery. Extensive home modifications are not required. https://orthoinfo.aaos.org/en/recovery/activities-after-hip-replacement/
Boo Chanco had been writing on Medical Tourism for years now, this is his latest.
https://www.philstar.com/business/2024/08/02/2374703/why-medical-tourism
My initial reaction to the news that we will now be promoting medical tourism was one of caution. Given the state of our medical care system and the chronic shortage of hospital beds, I am skeptical that medical tourism will be of real benefit to folks other than hospital owners.
The long lines at the admission section of most hospitals is a clear indication that medical tourism will only make things worse for us as foreign patients get priority. Hospitals, including the big ones, don’t have enough nurses so they usually block off a lot of rooms because they don’t have staff to provide the necessary service. We really don’t have hospital rooms to spare.
Still, there is no denying that medical tourism could be a foreign exchange earner for the economy. But we have formidable competitors among our neighbors who are already entrenched in the business. Besides, our local hospitals will have to get international accreditation.
Four Philippine hospitals have been cited by Joint Commission International Accreditation Standards for Hospitals (JCI) for rendering the best service to Filipino patients. They are Makati Medical Center and Asian Hospital for hospital program; The Medical City in Pasig City for hospital program and acute myocardial infarction; St. Luke’s Medical Center (SLMC) in Quezon City for academic medical center hospital program as well as for primary stroke.
JCI is a medical commission that helps international health-care organizations improve and demonstrate the quality of patient care. JCI’s accreditation and certification process is acknowledged by many medical organizations as essential in assuring a safe environment for their patients.
https://www.philstar.com/business/2019/03/06/1898913/medical-tourism/amp/
We have been hearing about government plans to promote medical tourism. But as one foreign consultant told me, we are ”not ready for medical tourism on a massive scale. You started back in about 2005 with bad advice and went downhill from there.”We apparently hired a medical tourism association, a group of two lawyers claiming to be experts. Then DOH and DOT in 2009, ”started buying conference stands to sell excess capacity in hotel rooms and hospital beds without having a product at a medical tourism event. Then came other conference organizers in 2010, 2011, 2012, and then another attorney posing as a medical tourism consultant and nothing…”Even as our efforts failed, Thailand, Malaysia, and Singapore successfully established a medical tourism sector. In our case, it was reverse medical tourism. The very rich among us go to Singapore, Thailand, and Malaysia for medical treatment and even annual check-ups.The Thai hospital group that was once with Asian Hospital could have helped us launch medical tourism, but they were gone too soon. We may have very good doctors, but the local medical community simply isn’t interested.Many countries make an effort to develop and promote medical tourism because there is a market. The high cost of treatment in the US makes an overseas trip for medical services a cost effective option.CNN had an article last month about India’s medical tourism industry that could grow by 200 percent by 2020, hitting $9 billion……..
I disagree that lhe local medical community “simply isn’t interested”. And I’m not proposing to promote “mass market” medical care, but profitable private hospital care.
I do note CNN’s finding that overseas services are indeed being taken up by Americans. Rather makes my case that there is a market even before Trump mucks with medical care in the US.
Here is Saint Paul’s international services program.
https://www.sph.org.tw/international-medical-service-en/international-medical-service/
Again duly noted with many thanks.
This is interesting as it corresponds with what Joey has written about Filipinos often trying to jump up the ladder and falling while trying to do it. It is different from the Karl Garcia approach that a (tennis) ball must first become a (pulot) boy before becoming a (tennis) player.
BTW any stats on medical tourists from Japan or Korea? The Philippines does have language tourists from Korea, born-again missionaries from Korea and Angeles bar owners from Korea. Are there Korean retirees like there are many American retirees? Obviously, retirees are not medical tourists, but they are an important clientele for the same hospitals as those that could serve medical tourists. I am asking about Korea/Japan due to their proximity.
Hospitals today provide “executive services” to expedite admissions and care for busy executives, and I would imagine foreign visitors arriving for significant medical problems would have (and pay for) such expedited care. I believe St Pauls already has such a program. My concept is not for routine patients and would not overload hospitals. Hospitals would welcome the profitable cases.
rich patients maybe given priority but care must not be expedited as there are tests that takes time to conduct. care is needed for best results, rush and there could well be repercussions. though we now have patients e health records available online and across the board so patients dont have to repeat their health histories every time they are admitted. though on doctors discretion, test may be repeated and patients re-interviewed and reassessed as health status can change drastically.
I am confident that hospitals run their executive programs competently.
OT. Today in History.. BTW, most of the women of Malolos who fought for a school for girls to be opened had Chinese-Filipino surnames.
In theory, Queen Isabel’s 1862 decree was to open two schools per town, one for boys and one for girls, in the Philippines, but the Spanish monks tasked with implementation often didn’t do it or opened only a school for boys. Though a generation later, some of those boys would be young men working in BPOs in Manila, correction as clerks and other workers in the booming businesses of Manila owned by Englishmen, Germans and Americans.. and though Rizal was against immediate independence, one particular group around a warehouseman for the German firm Fressel, Andres Bonifacio, wouldn’t be as patient, and the rest is again history.
The woman displayed in this picture died 80 years and 9 days ago. Her bones were only recently exhumed along with others from a mass grave under the Malate Catholic school. She was a resistance fighter and a scientist. Maria Orosa, most known as the inventor of banana ketchup. More educational opportunities for women materialized during American times, and even as the 1935 Constitution originally gave suffrage only to men who could read and write, there was a referendum pushed by Quezon himself soon after for suffrage. What also started in American times was Filipinas learning to be nurses, and yes, the venerable PGH is also a legacy of that era IIRC..
One could add that Maria Clara was exactly what Rizal didn’t want Filipinas to be, subservient and timid. Not just the letter to the women of Malolos confirms this, letters to his sisters from Germany that sound funny at first reading confirm this also. He wrote them that German women walk like men, and anyone who still saw in what stupor some probinsyanas still walked in the 1970s knows he wanted his sisters to be more purposeful, not so passive. One of his sisters even spoke English by the time Rizal was about to be executed. He gave her the lamp with his last poem in it and told her in English, which the Guardia Civil didn’t understand, that something was inside.
Filipinas seem not to be passive to me, today. Maybe WWII changed things, or television. Or the weakness of men. Maybe not weakness, maybe indolence and irresponsibility.
The 1970s definitely changed things a lot with people moving from the provinces to the city and yes, by the 1970s transistor TVs (my lolo’s cathode ray based TV that heated up on which I watched Marcos Sr. declare Martial Law after we had comics on TV for hours was too expensive for most Filipinos then, I recall how our Visayan gardener became a bit of a king in Balara when he bought a Sony TV and the entire neighborhood gathered in his place, one of the first to shift from wood and yero to hollow blocks, to watch Nora Aunor and Kuya Germs or Ike Lozada) and electrification of the provinces were a major shift. Among the elites, the hippie influence was strong, and my lolo gave up controlling his youngest daughter like he had all three elder sisters pass through very detailed interrogations and scared their suitors who felt like in a courtroom..
Most probably, Kris Aquino, who did many things her mother didn’t do, made things irreversible. 😉 Seriously, the Spanish idea of what women are to be was just an interlude considering the role of Filipinas before the Spanish conquest. And even after as for instance, an ancestor of President Duterte was an elite single mother in the late 19th century. At the end of the 19th century, Filipinas also could and did have businesses. Official Filipina feminism started in the American period, though, with the author Paz Marquez Benitez as a prominent example. She was also one of the first to write in English. Her short story Dead Stars is a classic.
you are right, joeam. filipino women cannot afford to lag behind their asian counterparts, and have learned to be breadwinners. husbands die, and like risa hontiveros, she became the family’s sole provider and brought up her 4 kids, the eldest is 18, the youngest is 9. as well, after her husband died, leni robredo become a single mother to her girls and at the same time, hold down a job.
maybe out of necessity, a number of single mothers are forging ahead sans partners. there are women who are home wreckers and steal husbands, as well as faithless husband that leave the marital home with nary a backward glance. so left behind with bills to pay and children to care for, many women cannot afford to wallow in self pity. they would have to find jobs and be self sufficient. sometimes luck is on their side, they have extended families and the support of the whole village that can help care for their children while women go to work.
ahem, it is alledged philmar alipayo, andi eigerman’s husband could not really stray, andi fought hard to get her man back and their lovely children have such a pull, philmar alipayo got back on track and back to andi. sadder maybe, but wiser.
“many women cannot afford to wallow in self pity”, perfect description of my wife who simply does not know how to be lazy. Through cold, headache, and fever, she works. And she can walk 8,000 steps taming the nearest mall.
your wife is a goddess!
Yes she is, and quite sparky, too, grand sense of humor, impossible to defeat in debate because she tends to start edging toward the knives and one is inclined to reflect that she comes from a family of murderers, in the Philippine tradition.
I believe that the school lasted only a few months, then closed down.
https://www.metropacifichealth.com/news/article/mvps-visionary-leadership-revolutionizing-healthcare-through-metro-pacific-health
https://healthwaymedicalnetwork.com.ph/
====
2 Medical Networks of two Rich Pinoys.
Their coopetition is very good news
Oh, excellent, excellent. MVP 21 private hospitals. Of course they could set up the scheme I’ve outlined. Simply do the housing, visa, and marketing aspects through the hub/BPO I’ve outlined and start bringing the ferreners and their money over.
Healthway is cancer specialized. A good resource to know.
I’ve looked at this before. One of the issues is people need family to heal effectively. that tilts the costs a lot
I was worried, too, but with room for saving $30,000 one can bring a friend or family member to assist. So I think it remains feasible.
friends and families can visit during visiting hours. they may not be allowed to stay over night, hospitals have strict rules. but there are pension houses or airbnb nearby where friends and relatives can elect stay by booking in advance.
incidentally, some children’s ward in private hospitals have ‘rest house’ in the hospital ground where parents can stay on doctors recommendation. rest house is for short and temporary stay only, and only available for parents who live far from the hospital. saves them the travel to and from. the house is run like a dorm with shared living spaces such as communal kitchen, bathroom and with access to wifi, etc.
other hospitals some are public also have emergency accommodation for close families of very sick patients who are not expected to live long. the accommodation is not advertised and very few knew about it. short stays can only be granted on doctors recommendation. the accommodation is often run by charity organisation and is free. though grateful relatives almost always give donation to the charity, the accommodation is meager and not luxurious.
Yes, good hospitals are sensitive to family needs. In Cebu, at least at Chong Hoa, you are required to have a ‘watcher’ stay with the patient in the room to assist as needed, even overnight. That’s a requirement that needs to go away as the bed for the watcher is just a bench, and it’s hard if kids are in school to have the spouse do that.
I stumbled into the hospital’s emergency accommodation by accident. my aunt had cancer and I was her carer. having stayed too long after visiting hours, I knew I missed the last train and may have to wait for the arrival of the earliest train at dawn. walking to the train station late at night and spending the night there alone and sleeping on the bench is scary. when a doctor asked me why I was crying, I told him my predicament. to my surprised, he asked a wardsman to escort me to the emergency accommodation designed specially for the likes of me, poor and lives far from the hospital, and cannot afford to hire uber to take me home.
the accommodation was behind the hospital, the old building that housed old medical equipment no longer usable, cordoned off. down the hall, old beds and mattresses were put to good use, instead of being thrown in the dumpster. the beds maybe saggy but the linens were clean. I counted ten beds and seven were already occupied. people wrought with sorrows, fearing for the outcomes of their sick relatives. no one talked. men and women were segregated, men in another section, women on the other. so few beds, no wonder the accommodation is kept secret. only those in direst of need can enter.
the hospital my aunt was in, discouraged stragglers in the corridors and in the wards. passageways must be kept clear and free of clutter in case of fire when all matters of mayhem can happen and people can get squashed. after visiting hours, a loud bell sounded, warning visitors to leave.
My my, what a night. Like from a Charles Dickens novel. It is somehow correct for the Philippines to have welcome accommodations, no matter what.